Brain Support Systems: Sleep, Insulin, and the Limits of Stimulant Stacks
What the evidence says about sleep architecture, intranasal insulin, and bioregulator peptides — and where the human data runs out.


Most "focus stacks" lean on the same lever: push dopamine and noradrenaline harder. Caffeine, modafinil, amphetamines, racetams, occasionally tianeptine — the unifying logic is that cognition is a stimulation problem. A more durable framing is that the brain is an energy-hungry organ whose performance depends on its support systems: sleep architecture, glucose handling, insulin signalling, autonomic tone, and cellular repair.1 2 None of those are pharmacologically sexy. All of them have stronger human evidence than the average nootropic.
This brief walks through three layers of that picture, ordered by how good the evidence is. Sleep is well-established. Intranasal insulin is promising and partly counter-intuitive. Bioregulator peptides (Pinealon, Epitalon, KED/EDR tripeptides) are mostly mechanistic and animal data — interesting biology, but not yet a human performance claim.
Sleep is the cleanest foundation
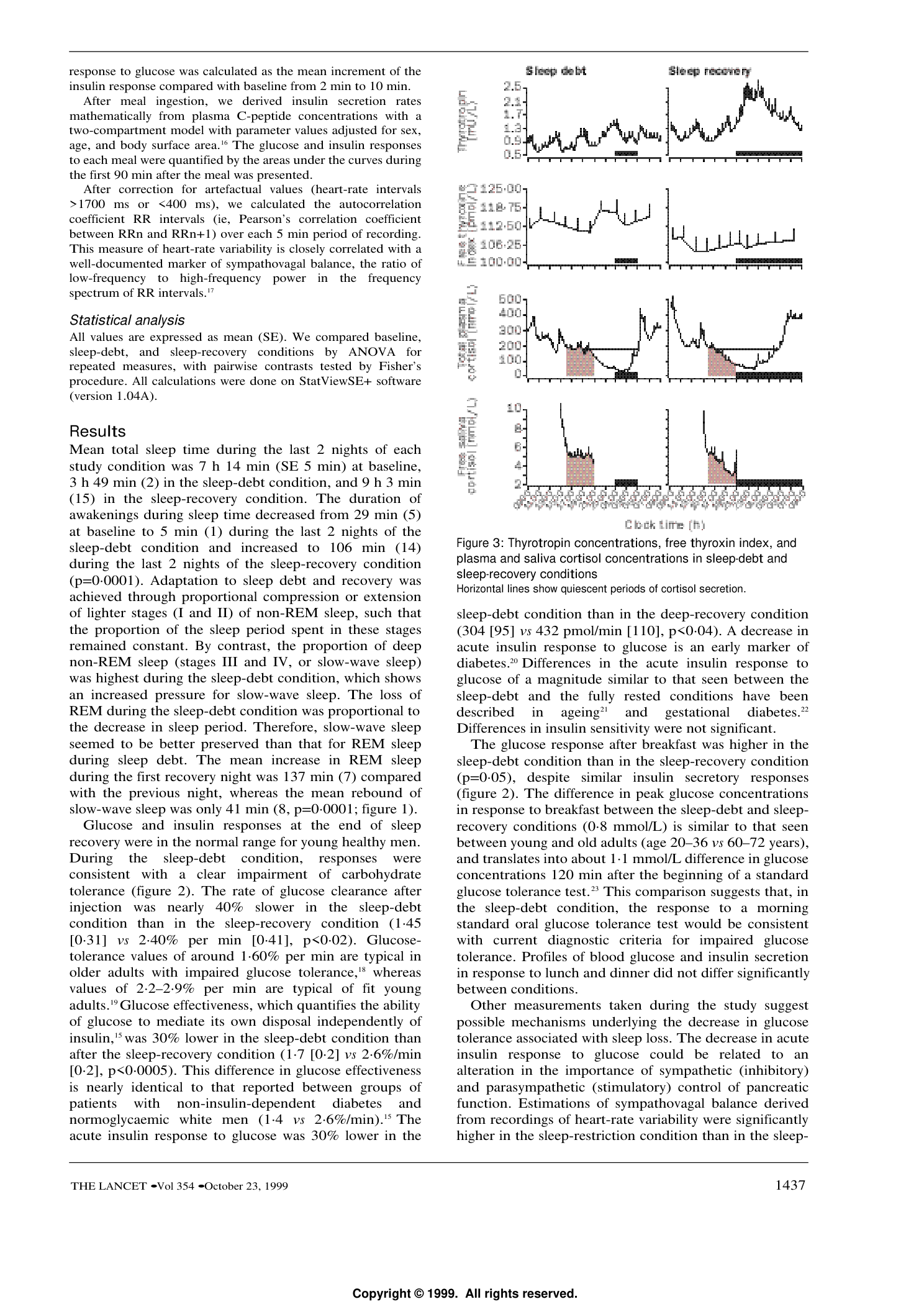
The Spiegel/Leproult/Van Cauter sleep-debt study remains the cleanest demonstration that short sleep degrades metabolism. After restricting healthy young men to four hours in bed for six nights and then recovering with twelve, the authors reported that glucose clearance was nearly 40% slower in the sleep-debt condition, glucose effectiveness was about 30% lower, and the acute insulin response to intravenous glucose was about 30% lower than after recovery.3
A 2022 systematic review and meta-analysis of randomised sleep-manipulation trials concluded that restricting sleep reduces insulin sensitivity across multiple measurement methods (OGTT, IVGTT, HOMA, hyperinsulinaemic-euglycaemic clamp).4 In the other direction, Leproult and colleagues found that extending sleep in chronically short-sleeping adults was associated with improved fasting insulin sensitivity, even without any other change in diet or exercise.5
The mechanistic supplement to all this is Xie et al.'s Science paper showing that interstitial space expands during sleep and metabolite clearance accelerates — sleep is not just rest, it's maintenance.6
The point isn't that sleep cures everything. It's that any cognitive intervention layered on top of chronic short sleep is fighting an upstream metabolic drag.
Intranasal insulin: a brain-side angle on memory
The intranasal route delivers peptides directly to the brain via olfactory and trigeminal pathways, largely bypassing systemic circulation.7 8 That matters because insulin has central nervous system effects — receptors are dense in hippocampus and hypothalamus — that the bloodstream can't easily access without spiking peripheral glucose.
Two human results anchor the cognition claim. Benedict et al. reported that eight weeks of intranasal insulin improved delayed word recall in healthy adults, with no measurable difference in blood glucose or plasma insulin between the insulin and placebo groups.9 Reger et al. reported that daily intranasal insulin in early-AD/MCI patients improved delayed verbal retention, attention, and functional status, again with fasting glucose and insulin unchanged.10 A 2023 systematic review and meta-analysis of human trials concluded that intranasal insulin produced small but consistent effects on memory and executive function, with the most reliable signal in older or insulin-resistant subjects.11
Kullmann et al.'s neuroimaging work shows the corresponding signal: intranasal insulin produces dose-dependent changes in resting-state brain activity and autonomic markers within hours.12
The "paradoxical" glucose-handling effect — and its caveats
Where it gets stranger is that pushing insulin into the brain seems to improve systemic glucose handling — not by adding insulin to the blood, but by routing through the central nervous system.
Heni et al. (2014) reported that intranasal insulin improved whole-body insulin sensitivity in lean men, with the effect linked to hypothalamic activity and parasympathetic outputs.13 Dash et al. found that intranasal insulin suppressed endogenous glucose production by roughly 35% compared with placebo, despite similar venous insulin concentrations.14 A follow-up by Heni et al. (2017) clarified the boundary condition: the lean-vs-overweight distinction matters, with the metabolic benefit blunted in overweight, obese, or brain-insulin-resistant subjects.15
A useful one-line frame: intranasal insulin may improve systemic glucose handling through central insulin signalling, hypothalamic/autonomic pathways, and reduced endogenous glucose production — but effects appear context-dependent and may be blunted in overweight, obese, or brain-insulin-resistant subjects.
The required caveat: a 2026 PET study by Latva-Rasku et al. observed brain-glucose-uptake effects from intranasal insulin in fasted lean men but did not see the corresponding peripheral tissue glucose-uptake change in that protocol.16 The authors note this doesn't necessarily contradict earlier work — prior effects may appear later or under hyperinsulinaemic-clamp conditions — but it's a real reminder that the central-to-peripheral pathway is sensitive to the experimental setup.
Insulin can also cause hypoglycaemia. Treating intranasal insulin as a self-experiment is not the same as a tracked clinical protocol.
Pinealon, Epitalon, and the bioregulator question
The Khavinson family of short peptides (KED/EDR, Pinealon, AEDG/Epitalon) has a research literature, but the strongest claims are made on cell and animal data, not human cognition trials. They belong in the brief because readers see them marketed; they don't belong on the same evidential tier as sleep or intranasal insulin.
The Pinealon rat work reports that offspring exposed to prenatal hyperhomocysteinaemia showed improved spatial-learning markers and reduced oxidative-stress signals in neurons when Pinealon was included.17 EDR/KED tripeptide work in a mouse Alzheimer's model reports preserved CA1 dendritic-spine density and reduced mushroom-spine elimination.18 19 These are neuroprotection / oxidative-stress signals — interesting biology, not a human performance claim.
For Epitalon, a 2025 cell-line paper reports dose-associated telomere lengthening in treated breast-cancer cell lines and significant increases in primary cells after a longer treatment period, with hTERT upregulation following Epitalon treatment.20 A separate cell paper reports that AEDG/Epitalon increased neurogenic differentiation markers in human gingival mesenchymal stem cells.21 This supports a cellular-repair / gene-expression / longevity-biology framing — and stops there.
If a brief on these compounds claims anything stronger than "promising mechanism, weak human evidence," it has overshot the data.
What to track in your own data
The pragmatic version of this is boring: if you want to test whether brain support systems matter for your cognition, you don't need a peptide. You need a fortnight of disciplined measurement.
A two-week baseline against a two-week intervention is enough to see signal in most wearable data. Useful columns:
- Recovery / HRV / resting heart rate — autonomic readiness and cardiometabolic stress.22 23
- Sleep performance and consistency — opportunity, execution, and circadian regularity.
- REM and slow-wave time — restorative architecture, not just total hours.
- Fasting glucose and post-meal peaks (if you wear a CGM) — the metabolic-support layer.
Wearable validation is real but partial. WHOOP's sleep estimates have been validated against polysomnography with reasonable agreement on totals and weaker agreement on stage-by-stage classification; HR and HRV from wrist PPG track ECG-derived references well at rest, less well during motion.22 23 24 Treat the device as a directional tracker, not a diagnostic.
The honest version of the upgrade is unglamorous: same stimulants you were using before, plus more sleep, more sunlight in the morning, an earlier last meal, and a CGM if you can get one. If those don't move the dial, layering peptides on top is unlikely to.
Reading checklist
When evaluating new "brain optimisation" claims, the methodology questions matter more than the molecule:
- Population — lean and healthy, or older/insulin-resistant? The intranasal insulin metabolic effect flips with body composition.15
- Endpoint — measured cognition (delayed recall, attention task) or self-reported focus? The latter is mostly placebo.
- Duration — single-dose, eight weeks, or chronic? Acute and chronic effects diverge.
- Comparator — placebo-controlled, or pre/post? Pre/post is hypothesis-generating, not evidence.
- Tier — human RCT, observational, animal, or cell? The bioregulator literature is mostly the last two; sleep is mostly the first two.
The more confident a vendor is in their molecule, the more likely the answer to those five is "we don't have that data yet."
References
- Attwell, D., & Laughlin, S. B. (2001). An energy budget for signalling in the grey matter of the brain. J Cereb Blood Flow Metab, 21, 1133–1145.
- Herculano-Houzel, S. (2011). Scaling of brain metabolism with a fixed energy budget per neuron. PLOS ONE, 6(3), e17514.
- Spiegel, K., Leproult, R., & Van Cauter, E. (1999). Impact of sleep debt on metabolic and endocrine function. The Lancet, 354, 1435–1439.
- Sondrup, N., Termannsen, A. D., Eriksen, J. N., et al. (2022). Effects of sleep manipulation on markers of insulin sensitivity: a systematic review and meta-analysis of RCTs. Sleep Med Rev, 62, 101594.
- Leproult, R., Deliens, G., Gilson, M., & Peigneux, P. (2015). Beneficial impact of sleep extension on fasting insulin sensitivity in adults with habitual sleep restriction. Sleep, 38(5), 707–715.
- Xie, L., Kang, H., Xu, Q., et al. (2013). Sleep drives metabolite clearance from the adult brain. Science, 342(6156), 373–377.
- Born, J., Lange, T., Kern, W., et al. (2002). Sniffing neuropeptides: a transnasal approach to the human brain. Nat Neurosci, 5, 514–516.
- Crowe, T. P., Greenlee, M. H. W., Kanthasamy, A. G., & Hsu, W. H. (2018). Mechanism of intranasal drug delivery directly to the brain. Life Sci, 195, 44–52.
- Benedict, C., Hallschmid, M., Hatke, A., et al. (2004). Intranasal insulin improves memory in humans. Psychoneuroendocrinology, 29(10), 1326–1334.
- Reger, M. A., Watson, G. S., Green, P. S., et al. (2008). Intranasal insulin improves cognition and modulates β-amyloid in early AD. Neurology, 70(6), 440–448.
- Wu, S., Stogios, N., Hahn, M., et al. (2023). Outcomes and clinical implications of intranasal insulin on cognition in humans: a systematic review and meta-analysis. PLOS ONE, 18(6), e0286887.
- Kullmann, S., Veit, R., Peter, A., et al. (2018). Dose-dependent effects of intranasal insulin on resting-state brain activity. J Clin Endocrinol Metab, 103(1), 253–262.
- Heni, M., Wagner, R., Kullmann, S., et al. (2014). Central insulin administration improves whole-body insulin sensitivity via hypothalamus and parasympathetic outputs in men. Diabetes, 63(12), 4083–4088.
- Dash, S., Xiao, C., Morgantini, C., et al. (2015). Intranasal insulin suppresses endogenous glucose production in humans compared with placebo in the presence of similar venous insulin concentrations. Diabetes, 64(3), 766–774.
- Heni, M., Wagner, R., Kullmann, S., et al. (2017). Hypothalamic and striatal insulin action suppresses endogenous glucose production and may stimulate glucose uptake during hyperinsulinemia in lean but not in overweight men. Diabetes, 66(7), 1797–1806.
- Latva-Rasku, A., et al. (2026). Intranasal insulin affects brain, but not peripheral tissue, glucose uptake in lean, healthy men: a PET study. Am J Physiol Endocrinol Metab.
- Arutjunyan, A. V., Kozina, L. S., Stvolinskiy, S. L., et al. (2012). Pinealon protects the rat offspring from prenatal hyperhomocysteinemia. Int J Clin Exp Med, 5(2), 179–185.
- Kraskovskaya, N. A., Kukanova, E. O., Lin'kova, N. S., et al. (2017). Tripeptides restore the number of neuronal spines under conditions of in vitro modeled Alzheimer's disease. Bull Exp Biol Med, 163, 550–553.
- Khavinson, V., Ilina, A., Kraskovskaya, N., et al. (2021). Neuroprotective effects of tripeptides — epigenetic regulators in mouse model of Alzheimer's disease. Pharmaceuticals, 14(6), 515.
- Al-Dulaimi, S., Thomas, R., Matta, S., & Roberts, T. (2025). Epitalon increases telomere length in human cell lines through telomerase upregulation or ALT activity. Biogerontology, 26(5), 178.
- Khavinson, V., Diomede, F., Mironova, E., et al. (2020). AEDG peptide (Epitalon) stimulates gene expression and protein synthesis during neurogenesis. Molecules, 25(3), 609.
- Miller, D. J., Lastella, M., Scanlan, A. T., et al. (2020). A validation study of the WHOOP strap against polysomnography to assess sleep. J Sports Sci, 38, 2631–2636.
- Bellenger, C. R., Miller, D. J., Halson, S. L., et al. (2021). Wrist-based photoplethysmography assessment of heart rate and heart rate variability: validation of WHOOP. Sensors, 21(10), 3571.
- Miller, D. J., Sargent, C., & Roach, G. D. (2022). A validation of six wearable devices for estimating sleep, heart rate and heart rate variability in healthy adults. Sensors, 22(16), 6317.
Nothing on this page is medical advice. Intranasal insulin and peptide / bioregulator products are investigational or off-label in many jurisdictions and should be discussed with a qualified clinician — insulin can cause hypoglycaemia, and peptide-product quality and regulatory status vary widely.